APD

As individual as your patient - Automated peritoneal dialysis with sleep•safe harmony
The prescribing information for Peritoneal Dialysis solutions can be viewed here.
Why automated peritoneal dialysis (APD)?
APD uses a programmable machine, or cycler, that controls the volume, filling, dwell time and drainage of the solution. Thanks to automated dialysis, patients can be dialysed at home, even when sleeping.
As APD is offering more free daytime, it is a PD technique with obvious advantages for patient’s lifestyle. Patients may pursue a job and have more time for personal and family activities.1
Finally, APD cyclers offer a variety of individualisation options for the treatment, allowing you to even better consider the needs of your patient, supporting you to improve patient care.
![[Translate to English (GB):] APD - man reading on a bed](/fileadmin/data/masterContent/images/New_HCP_Content/fmc_1346_4x3.jpg)
In APD our sleep•safe harmony cycler offers advanced features, all aimed at improving patient care.
- Increased treatment flexibility with FlexPoint technology2
- Integrated on-screen animations give guidance and facilitate setup2
- As proposed by Fischbach et al., potentially improved ultrafiltration (UF) as well as clearance of urea, creatinine, phosphate, and sodium, with individually adapted APD (aAPD)3
- Advanced fluid management information package available as fluid management aims to better control the patient’s fluid status in order to improve longterm technique and patient survival4
Getting started with education in APD – The difficult part was making it easier
FMC created training solutions that focus on conveying the information that really matter and offers support in preparing and setting up the treatment.
Train
- Training videos for caregivers and patients to support training
- Start with supportive extra training material for our APD devices
- Set of patient information materials to support you in training the patient
Start
- Support in planning and preparing the therapeutic home environment
Our products - Key features of the sleep·safe harmony
sleep·safe harmony offers features aimed at improving patient care. It also provides training support by guiding on-screen animations directly on the device.
- Create prescriptions directly on the device
- On-screen keyboard
- Improved fluid usage – no extra volume for priming
- Permitted patient volume – the maximum individual fill volume
- Permitted residual volume – the maximum individual volume that may remain in the patient’s peritoneal cavity
- The goal is to:
- Reduce potential outflow alarms for a more quiet and restful sleep
- Maintain the prescribed treatment time
- Improve treatment effectiveness
- Provide more flexibility in treatment execution within defined individual limits to improve patients’ well-being and safety
- Automatic connection and barcode recognition of bags
- Integrated handles
- PatientCardplus capable of storing up to nine different prescriptions and more than 12 months of treatment data
- Automatic inline flow heating of the dialysis solution to body temperature directly during the inflow phase - no need to preheat the solution bag upfront/in advance of the treatment
- Automatic draining feature – the solution bags and the line set are drained automatically, no manual handling needed
- Plug & use – no transformer needed due to double installation
- Guiding animations directly on the device
- Large touch screen
- sleep•safe harmony system daily disposables are made of PVC-free and plasticiser-free materials such as Biofine (Except APD drainage options)
![[Translate to English (GB):] sleep safe harmony](/fileadmin/data/masterContent/images/New_HCP_Content/sleep-safe-harmony.jpg)
Adapted APD (aAPD) is one way to personalise treatments
Using sleep•safe harmony, the prescription can be individualised on several levels:
- Infusion volume
- Dwell time
- Glucose profile
- Calcium profile
- Different solutions per cycle within the same treatment
- FlexPoint
Because every patient is different: aAPD – Fischbach et al.2 suggests potential better ultrafiltration and clearance within a 9 hour treatment totalling 12000ml fill volume, in comparison to CAPD, .2
Your patients have a chronic disease in common, but differ in many ways: age, height, weight, stage of illness, residual kidney function etc. These differences have a decision impact on the PD treatment required.
Patients’ needs are different:
Age is an important factor influencing the choice of dialysis modality. Patients with good dexterity and motivation are good candidates for PD. With increasing age, the associated comorbidities of dialysis patients might deteriorate and with it their frailty.
Management of weight is an important success factor in PD patients. Changes in weight due to lifestyle, calorie intake, disease and hydration status need constant monitoring and adaptation of PD therapy.
Dialysate to plasma ratio is a common measure used to evaluate peritoneal transport characteristic in PD patients. Patients can be categorised into high (fast), high average and low (slow) transporters based depending upon the status of their peritoneal membrane. Peritoneal membrane transport characteristics change with time on PD. Therefore, regular monitoring of D/P creatinine and subsequent adjustment of PD prescriptions is recommended.
Patients are classified into high (fast), high average and low (slow) transporters based on the function of their peritoneal membrane. With time and increasing duration of stay on PD, patients tend to become fast transporters. PD prescriptions need to be adapted according to patients' transport status for an optimal patient outcome.
RKF has an impact on patient survival and quality of life of PD dialysis patients. Its longer preservation is a major advantage. Thus, interventions to preserve RKF, like prescription of biocompatible PD fluids, are important.
Due to compromised kidney function, bodies' own capacity to remove excess fluid also diminishes and patients need dialysis to generate UF. The amount of UF needed varies depending upon many factors, like lifestyle, disease progression and other comorbid conditions. An adequate UF is therefore critical for successful PD.
Kt/V urea is urea clearance normalized to total body water. It is an important parameter to check PD adequacy. A total Kt/V urea of at least 1.7 per week is recommended for PD patients.5
![[Translate to English (GB):] APD study](/fileadmin/data/masterContent/images/New_HCP_Content/aAPD_1_crop.jpg "A representation of the aAPD method described by Fischbach M. et al., (2011)")
A representation of the aAPD method described by Fischbach M. et al., (2011)
Fischbach study supports aAPD2
Fischbach M. et al. conducted a randomised, prospective, cross-over, multicenter study. Nineteen patients were included in the final analysis.
According to Fischbach et al., aAPD offers better results using the same time and resources2
- aAPD is possible without extra fluids or a longer amount of time
- Efficiently uses existing treatment resources: better ultrafiltration and clearance with same 1.5% glucose Peritoneal Dialysis solution, 12000ml fluid volume and 9 hour treatment time compared to conventional APD (cAPD)
Attaining adequacy targets
The aAPD approach was proposed by Fischbach M. et al.2 By combining sequences of short dwells and small fill volumes with long dwells and large fill volumes, aAPD aims to promote UF and clearance within one PD session. The blood purification and UF achieved for every gram of glucose absorbed was higher in aAPD in comparison to cAPD.
The challenges of PD – Reaching adequacy targets
Reaching adequacy targets in PD for both UF and clearance is challenging. Fischbach et al. propose that shorter dwell times and smaller fill volumes promote the process of UF, while longer dwell times and large fill volumes increase solute clearance.2 The proposed strategy may have the potential to improve the two targets within one PD session.
cAPD
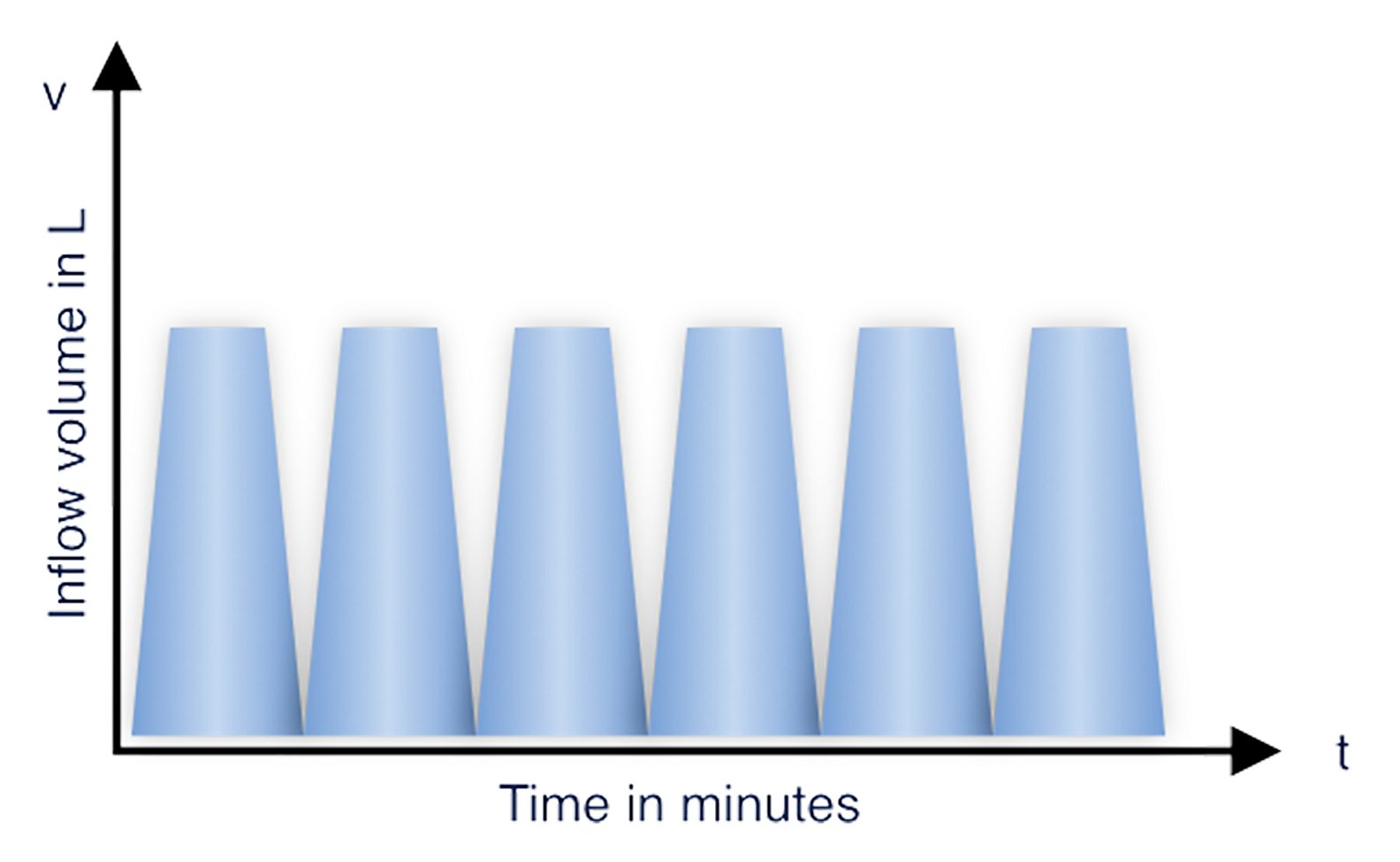
Figure 1: Modified cAPD graphic following Fischbach M. et al. 2011
aAPD
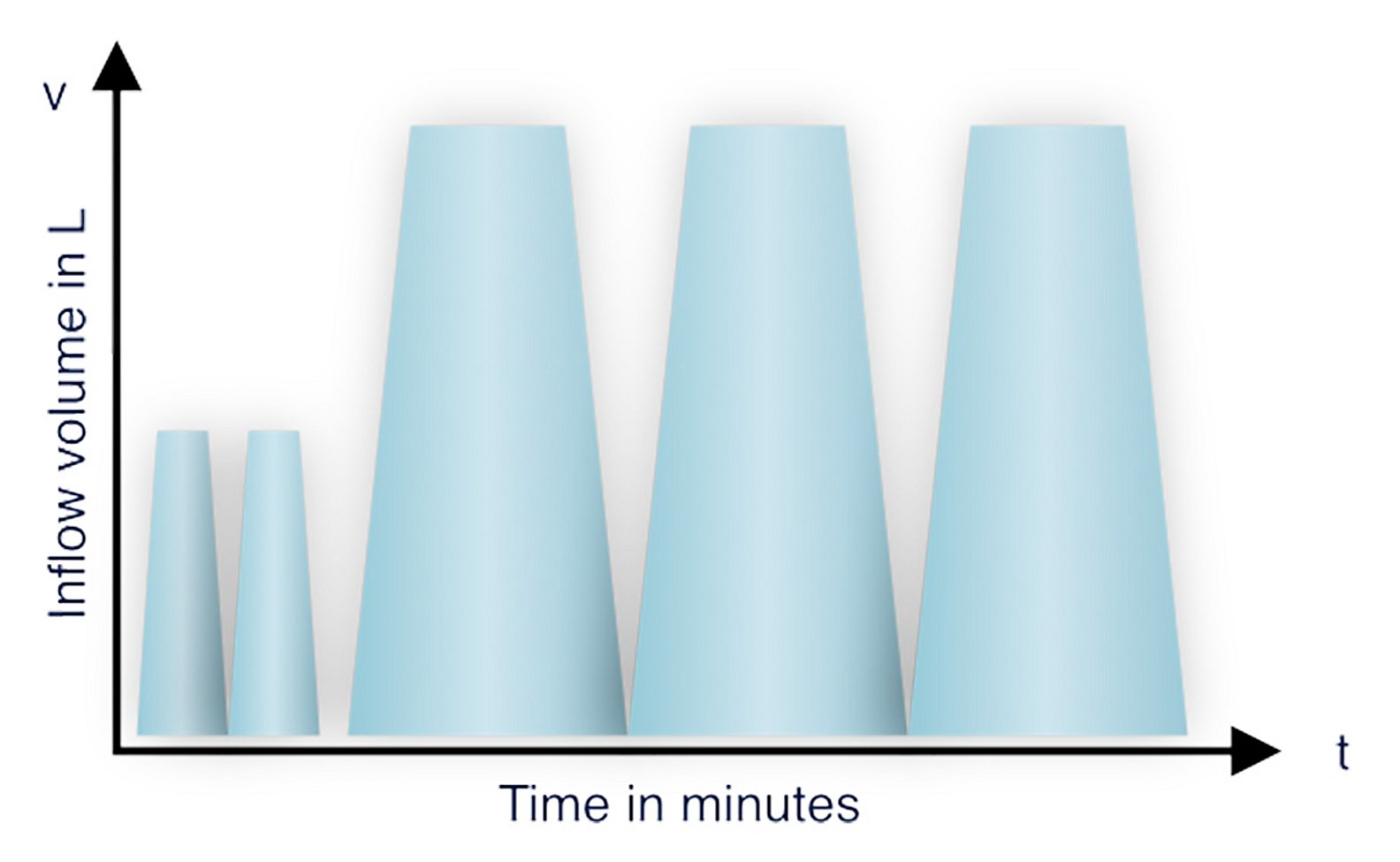
Figure 2: Modified aAPD graphic following Fischbach M. et al. 2011
Adapted APD is possible without extra fluids or a longer amount of time, with the same glucose concentration.
Summary of potential patient benefits as reported by Fischbach et al2
Patient benefits
- Improves ultrafiltration
- Better sodium removal
- Lower blood pressure
- Promotes clearance: urea, creatinine, phosphate
- Reduced metabolic load
Clinical value
- Improved use of existing treatment resources: better ultrafiltration and clearance with same 1.5% glucose Peritoneal Dialysis solution, 12000ml fluid volume and 9 hour treatment time compared to cAPD
APD monitoring and support
Smart digital tools offer convenience for patients and caregivers in the comfort of the patients’ homes.
Support
- A simple ordering process in combination with personal phone support ensures that patients can order materials anytime and anywhere
- The delivery service ensures that PD solutions and disposables are delivered straight to your patient’s doorstep
- The PD travel service enables patients to continue travelling as the required goods are directly sent to the patient’s holiday destination*
Monitor
- Streamlined PD therapy management through easy accessibility to therapy information via our PatientOnLine tool
* The service is not available in all countries. The availability of the service and products must be clarified before planning or booking a vacation.
![[Translate to English (GB):] Peritoneal dialysis - woman with child lying in bed](/fileadmin/_processed_/a/c/csm_harmony_woman_child_bfe0b02558.jpg)
![[Translate to English (GB):] CAPD - reading woman](/fileadmin/_processed_/1/7/csm_fmc_1434_7505495415.jpg)
References
1 Roumeliotis A et al. Int Urol Nephrol 2021; 53(6):1149-1160
2 Punzalan S et al. Journ of Kidn Care 2017; 2(5):262-267
3 Fischbach M et al. Peritoneal Dial Int 2011; 31(4):450-458
4 Ronco C et al. Nephrol Dial Transplant 2015; 30(5):849-858
5 Tzamaloukas AH et al. Semin Dial 2008; 21(3):250-257